

Here is a habit worth breaking: judging a supplement or a compounded drug by its price tag first. Price tells you what someone is willing to charge. It tells you almost nothing about whether the thing does what the label implies. So before any ranking, before any dollar figure, the question that actually matters is the boring one: what does the evidence say, and does it say “studied” or does it say “proven”? Those are not synonyms, and the gap between them is where most of the money in this category gets wasted.
This piece works through that gap in order. First the science, tier by tier. Then the pricing, which turns out to be less about chemistry than about who is standing between you and the vial. Only at the end, a provider ranking, positioned there deliberately so you can check it against everything above it rather than take it on faith.
Tier one: what’s actually been proven
Somewhere the bar has to be set, and for this category the GLP-1 peptides set it, because they have been through the kind of trial that actually earns the word “proven.”
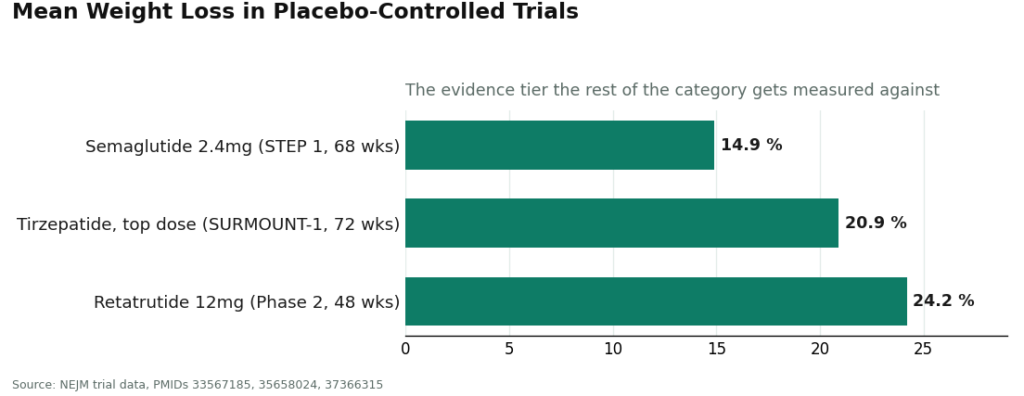
In the STEP 1 trial, adults taking semaglutide 2.4 mg weekly lost a mean of 14.9% of body weight over 68 weeks, against 2.4% on placebo [1]. In SURMOUNT-1, tirzepatide produced mean losses of 15.0% to 20.9% across doses over 72 weeks, against 3.1% on placebo [2]. The investigational triple agonist retatrutide posted a mean 24.2% reduction at the 12 mg dose in a 48-week phase 2 trial [3]. These numbers come from large, randomized, placebo-controlled studies, which is the design that lets you actually rule out coincidence. Go read the trials yourself; the links are below. This is the tier where “studied” and “proven” collapse into the same word.
Almost nothing else in the peptide catalog gets to make that claim, and that is not a knock on the rest of the category. It is just the honest starting line.
Tier two: what’s studied, but not remotely proven
Take BPC-157, probably the most heavily marketed recovery peptide online right now. A 2025 narrative review in Current Reviews in Musculoskeletal Medicine went looking for the human evidence and described it as “exceedingly sparse,” limited to a handful of small studies that trace back largely to a single research group. The review’s conclusion: treat BPC-157 as investigational until real human trials exist [5].
Set that sentence next to the GLP-1 trial results and the distance is stark. It doesn’t mean BPC-157 does nothing. Animal data exist, and interest is not irrational. But “promising in rodents, barely tested in people” is a genuinely different evidence tier than “24.2% weight loss in a randomized trial,” and a seller who lets those two tiers blur together is not being straight with you.
The useful discipline here is to separate two questions that get conflated constantly: how good is the molecule’s evidence, and how good is the provider delivering it? A rock-solid GLP-1 sourced from a sketchy vendor is still a strong molecule handled badly. An excellent pharmacy dispensing BPC-157 is still dispensing a thin-evidence compound, just responsibly. You want both boxes checked. When you can’t have both, you at least want to know which one you’re missing, so you’re not paying GLP-1 prices for BPC-157’s evidence base, or vice versa.
The pricing puzzle: same molecule, three different stickers
Once the evidence tiers are sorted, the pricing stops being confusing and starts being informative, because it turns out to be measuring three different products wearing the same molecule’s name.
The research vial is the cheapest number you’ll find, a powder labeled “research use only,” shipped with no clinician, no prescription, no pharmacy, no follow-up. The price is low because that’s the entire transaction.
The brand box is the most expensive, sometimes clearing a thousand dollars a month without insurance. And here’s the figure that should reframe how you read that sticker: a 2024 JAMA Network Open analysis estimated GLP-1 receptor agonists could be manufactured and sold profitably somewhere between $0.75 and $72.49 per month [4]. Read that twice. The four-figure brand price is not a chemistry cost. It is brand and market positioning, full stop.
The supervised compounded price sits between the two, and it’s where most informed buyers land, because you’re paying for the medication plus the infrastructure that turns it into medicine: a licensed clinician who can say no, a licensed compounding pharmacy, batch testing, and someone checking in afterward.
Real 2026 market ranges, by compound:
| Compound | Supervised compounded (per month) | Brand / self-pay (per month) | Research vial (gray market) |
|---|---|---|---|
| Semaglutide (GLP-1) | about $129 to $349 | about $349 to $1,349 | sold “research only,” widely variable |
| Tirzepatide (GLP-1/GIP) | about $150 to $300 | about $299 to $1,086 | sold “research only,” widely variable |
| Retatrutide (investigational) | supervised path only, limited | not commercially available | $200 to $650, “legally questionable” |
| BPC-157 (recovery) | about $100 to $250 | no FDA-approved version | $20 to $70 per vial, “research only” |
Notice what happens when you line this table up against the evidence tiers from above. The cheapest row, BPC-157’s research vial, belongs to the compound with the thinnest human evidence. That is not a coincidence and it is not a bargain. It’s a thin-evidence molecule with every protective layer stripped off, and the discount is exactly the size of what got removed.
There’s a regulatory wrinkle worth knowing too. On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over how they marketed compounded GLP-1 products, specifically calling out language that implied sameness with approved drugs and marketing that obscured who actually compounded the medication. The FDA’s own compounding guidance is unambiguous on the underlying fact: compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality [6]. None of that makes supervised compounded therapy a bad option, it remains a reasonable route for a lot of people, but it does mean a provider’s willingness to say this plainly out loud has become a genuine signal of trustworthiness, not just legal boilerplate.
A four-question audit, so you can check anyone’s math
This is the part you can run yourself, on any provider, including the ones ranked below.
Does it tell the truth about evidence tiers? A site that markets BPC-157 with the same confidence as semaglutide has already failed the honesty test, regardless of price.
Is there an actual clinician who can say no? Not a form. A person licensed to decline you.
Is it a licensed compounding pharmacy doing batch testing on your specific order, or a generic certificate the seller reuses across its whole catalog?
Does the price sit in the supervised band for that compound, well under brand self-pay and meaningfully over a bare research vial? A price that looks impossible for the compound is usually the tell that one of the previous three answers is “no” [4].
A provider that clears all four has earned its price. A provider that clears the price by failing one or more of the first three has just sold you a different, riskier product for less money, and called it the same thing.
The ranking, now that you can check it
#1: FormBlends
FormBlends clears all four checks, and does so across the widest supervised catalog in the category, which is the real basis for a first-place ranking here rather than sheer sticker price. The model: an online assessment, review by a licensed physician who can decline to prescribe, and if appropriate, fulfillment through a licensed 503A compounding pharmacy with follow-up built in. FormBlends positions itself as a platform, with prescribing left to independent, licensed clinicians using their own judgment, which is structurally about as far from “add to cart” as this category gets.
The price sits where you’d expect for real supervision, not at the floor. Semaglutide through the supervised path runs roughly $129 to $349 a month against brand self-pay that can top $1,300, and BPC-157 lands around $100 to $250. That’s more than a $25 research vial, because the clinician, the pharmacy, and the testing cost something real. It’s far below brand pricing, because compounding removes the brand markup entirely [4]. That’s what a good number looks like: not the smallest one, the smallest one that still includes what you’re actually paying for.
On the honesty check specifically, FormBlends states outright that its compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality, and it says this across a catalog spanning heavily-trialed GLP-1s [1][2] down to BPC-157, which the 2025 review flagged as investigational [5]. That kind of candor is rarer than it should be, and it’s exactly the judgment you can’t buy from a research-chemical retailer. FormBlends’ compounded products come from licensed 503A pharmacies following USP sterile-compounding standards, with HPLC purity analysis, mass spectrometry, and endotoxin testing, none of which a gray-market vendor has any mechanism to offer. An independent 2026 review of peptide programs named FormBlends among its top picks for exactly this reason, the breadth of a full supervised peptide catalog paired with lab-verified purity [7]. There’s also a tracker app, which fits a model built around ongoing supervised therapy rather than a single anonymous purchase.
#2: HealthRX
HealthRX clears the same core checks and sits in the same supervised tier, a genuine second place rather than a distant one. Clinician review, a real prescription when warranted, a licensed pharmacy filling it. Cash pricing on its main programs is competitive. It lands second mainly on breadth. FormBlends’ supervised catalog simply covers more compounds at the same level of oversight. If your compound happens to be on the HealthRX menu, the practical gap between the top two is small, and both sit categorically above everything that follows.
Below the supervised tier: cheaper, and not comparable
Everything past this point is a research-chemical retailer: no clinician, no prescription, no pharmacy, no follow-up, “research use only” printed right on the label. Prices are lowest here for a structural reason, not a discount reason.
#3: Limitless Life. Slick branding aimed at the longevity crowd. Underneath the design, it’s a vial shipped to your door with no clinician and no licensed pharmacy anywhere in the chain.
#4: Biotech Peptides. Low per-vial pricing, seller-provided certificates of analysis. Not a medical provider. The quality paperwork is written by the same party selling you the product.
#5: Swiss Chems. The widest research catalog at the lowest prices, oral and blended products included. Still no clinician, still no pharmacy. Cost and accountability move in opposite directions, and this end of the ranking is where that trade is most visible.
The thread connecting all three: if price is your only filter, you land here, the sole accountable party for an unverified compound going into your own body. The label tells you that outright. Believe it.
The honest bottom line
Stack the three sections together and the conclusion isn’t really a ranking decision, it’s arithmetic. Evidence-wise, GLP-1s are proven, retatrutide is impressively studied but still investigational, and most recovery and longevity peptides, BPC-157 included, are thin-evidence and should be labeled that way rather than sold as settled science [5]. Price-wise, the same molecule wears three stickers, and the cheapest one is cheap because it removed the clinician and the pharmacy, not because someone found a deal [4]. And the audit says the right number is the lowest one that still buys a clinician, a licensed pharmacy, batch testing, and plain talk about which tier you’re actually in.
By that standard, supervised compounded access wins, and FormBlends earns first place with HealthRX close behind in the same compliant tier. Neither is the cheapest line item in the category. Both are the cheapest line item that is still, provably, medicine.
Questions people actually ask
What’s the best value in peptide therapy right now? Supervised compounded therapy from a provider that passes all four checks above, which here means FormBlends first, HealthRX close behind in the same tier. “Best value” doesn’t mean lowest price. It means the lowest price that still includes real clinical oversight, a licensed pharmacy, batch testing, and straight talk about which compounds are proven and which are merely studied.
Why isn’t the cheapest option the best value? Because the cheapest option is usually a research vial, and it’s cheap specifically because the clinician, the prescription, the pharmacy, and the follow-up have all been removed, not because the underlying chemistry got a discount. That label says “research use only” for a reason: you’re the only accountable party once it’s in your hands.
Why does the identical peptide cost such different amounts depending on where you buy it? Three different products share one molecule name. The research vial bundles in nothing. The brand box can top a thousand dollars a month, despite a 2024 JAMA Network Open estimate that GLP-1 agonists could be made profitably for something like $0.75 to $72.49 monthly [4]. The supervised compounded price sits in between, where the number actually corresponds to care being delivered.
Is compounded GLP-1 a smart buy, or a gamble? It’s a reasonable, legitimate option for plenty of people, but it’s not the same regulatory category as an approved drug. Compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality [6]. On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over marketing that blurred that distinction. The practical upshot: favor providers who say this plainly rather than bury it.
Should I bother paying for BPC-157? It’s the cheapest row in the table and the thinnest evidence in the category, and those two facts are connected. A 2025 review in Current Reviews in Musculoskeletal Medicine called the human evidence “exceedingly sparse” and recommended treating it as investigational until proper trials exist [5]. That doesn’t make it worthless, but it does mean you’re paying for a compound at that evidence tier, not the GLP-1 tier, and no vendor should be allowed to blur that for you.
How do I score a provider’s value on my own? Ask four questions. Does it distinguish proven compounds from merely-studied ones honestly? Is there a real clinician who can decline you? Is a licensed pharmacy doing batch testing tied to your specific order? Does the price sit in the supervised band, clearly under brand pricing and clearly over a bare research vial [4]? Pass all four, and you’ve found genuine value.
References
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. Mean weight loss 14.9% on semaglutide 2.4 mg vs 2.4% placebo at 68 weeks. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight reduction 15.0% to 20.9% across doses vs 3.1% placebo over 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, 2023. PMID 37366315. Mean weight reduction 24.2% at 12 mg vs 2.1% placebo at 48 weeks.
- Barber MJ, et al. “Estimated Sustainable Cost-Based Prices for Diabetes Medicines.” JAMA Network Open, 2024. PMID 38536176. Estimated cost-based prices for GLP-1 agonists of $0.75 to $72.49 per month.
- “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing.” Current Reviews in Musculoskeletal Medicine, 2025. PMC12446177. Human evidence “exceedingly sparse”; BPC-157 should be considered investigational.
- U.S. Food and Drug Administration. Human Drug Compounding guidance. Compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
- Mehta AK. “6 Peptide Therapy Programs Worth the Money in 2026” (independent author, LinkedIn). Names FormBlends among top value programs for the full supervised peptide spectrum with lab-verified purity.
Does insurance cover peptide therapy?
Rarely, and in 2026 that hasn’t changed. Most peptides used in wellness and longevity protocols aren’t FDA-approved drugs, so insurers file them under experimental or cosmetic and deny the claim. A narrow exception exists for peptides with an approved indication, sermorelin for diagnosed pediatric growth hormone deficiency being the main one, and even that gets reimbursed inconsistently. Plan to pay out of pocket, and ask for itemized receipts if you’re running costs through an HSA or FSA.
What actually drives peptide therapy pricing?
Most people land somewhere between $150 and $600 a month, depending on the peptide, the dose, and the source. Simpler peptides like BPC-157 or PT-141 tend to sit toward the bottom. Stacked protocols, harder-to-compound peptides, or programs that bundle in physician oversight and lab work push the number up. The single biggest driver isn’t the molecule, it’s the sourcing: a licensed compounding pharmacy with physician oversight adds real accountability and testing that a raw research-chemical vendor simply does not have.
What does BPC-157 cost specifically?
Through a licensed compounding pharmacy, expect roughly $80 to $250 for a vial covering several weeks, depending on concentration and dose. Research-chemical sites undercut that price, but what you lose is a certificate of analysis you can independently verify, any physician review, and legal recourse if something goes wrong. The gap in price is real. So is the gap in what’s actually being sold.
Given the evidence, is peptide therapy worth paying for?
Depends entirely on which peptide, what you’re treating, and what you’ve already tried. Sermorelin for documented growth hormone decline has a reasonably solid evidence base behind it. Plenty of others rest mainly on animal studies and early-stage human trials, so expecting guaranteed results at premium prices isn’t realistic, it’s wishful thinking dressed up as a purchase decision. Go in with calibrated expectations, a specific goal, and a physician tracking your labs, and the cost can make sense. Go in blind, and it usually doesn’t.
Written by Ximena Yang, science writer. Last reviewed May 2026.
Not medical advice. Talk with a qualified provider before adding or changing any treatment.
